

The TIF® procedure fixes the root cause of reflux.
TIF trained physicians are able to restore the natural shape, location and effectiveness of your esophageal valve with an innovative procedure, stopping reflux.
The vast majority of patients experience little discomfort post-procedure. After the healing period of four to six weeks, they are off daily PPIs and back to their healthy state once more.
Benefits
- Minimally invasive
- Fast recovery
- No incisions
- FDA cleared
- No increased flatulence
- Exemplary safety profile
- No increased bloating
- Covered by most insurance
- No metal implant
- Controls disruptive symptoms
No Incisions Makes Every Body Happy
Advancements in fundoplication techniques have evolved the traditional reflux surgery from a major open operation to a TIF procedure: incision-free and without the negative side effects of traditional reflux surgery.
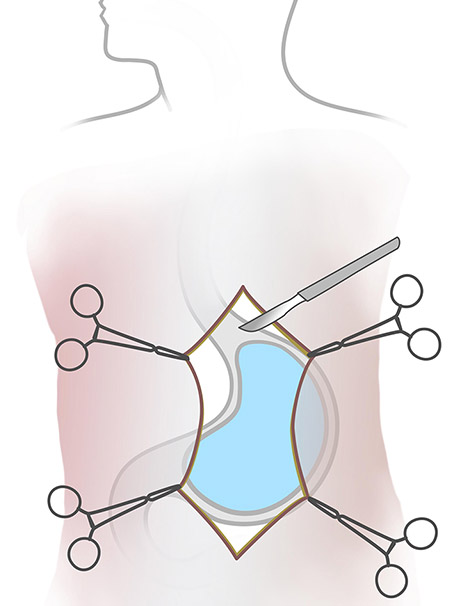
- Major surgery with large incision
- Esophagus is wrapped 360°
- Some patients cannot belch or vomit
- Long recovery
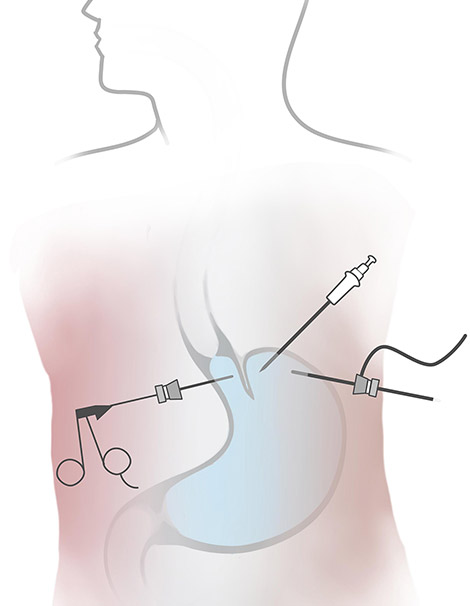
- Major surgery requiring several incisions
- Esophagus is wrapped 360°
- Some patients cannot belch or vomit
- Long recovery
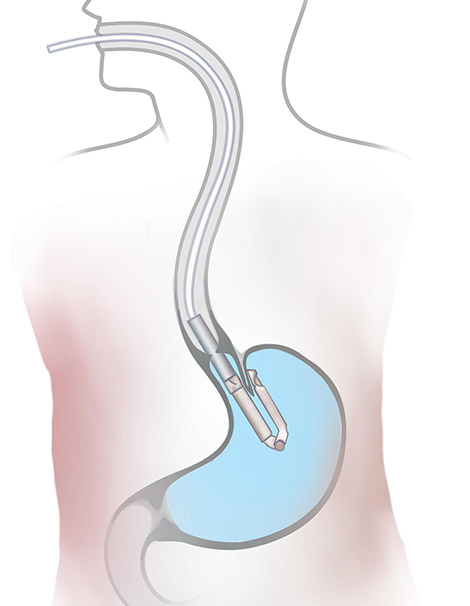
- Device uses oral pathway, no incisions needed
- Esophagus partialy wrapped 270-300º
- Allows for belching and vomiting
- Short recovery
Answer a few questions about your reflux and take advantage of a free consultation with a registered nurse. |
 |
Comparing Traditional and Laparoscopic Fundoplication with the TIF procedure
TRADITIONAL
Results of a full wrapping of the esophagus.
Some patients experience:
- Difficulty swallowing
- Increased bloating
- Increased flatulence
- Inability to belch
- Inability to vomit

THE TIF PROCEDURE
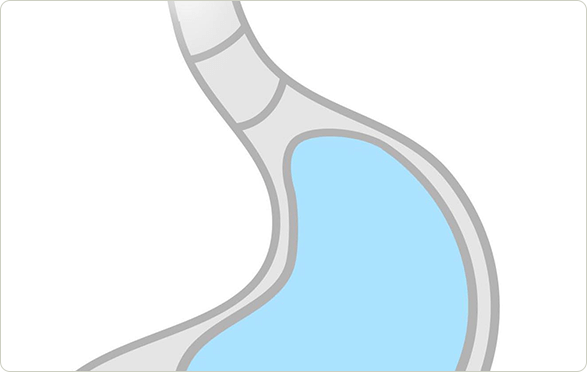
Results of a partial wrap of the esophagus:
- Restores the valve to its natural state
- No incisions, no cutting of body tissues
- No implants
- No negative long-term side effects
- Faster recovery time.
Incision-free Surgery? Yes!
The TIF procedure takes advantage of advancements in minimally invasive procedures to restore your esophageal valve. TIF trained physicians use an endoscopic device that enables them to reach the valve and stomach without the need for incisions.

Why cut if you don’t have to?
The TIF procedure eliminates the need for cutting stomach tissue by approaching the valve through the mouth using a flexible, camera-equipped, single use device.
First, the TIF procedure lengthens the esophagus. Then the top of the stomach is gently folded and partially wrapped around the lower esophagus. It is held in place with fasteners made of benign material physicians have used inside the body for decades. No cutting needed.
“The TIF procedure is literally the only operation that I’ve done in the past several years where we’re actually high-fiving after the operation because it looks so good.”
—Dr. Keith Goldberg, M.D.,
Surgical Alliance Middle Tennessee
NorthCrest Health Medical Center
Find a TIF trained physician near you.
The TIF Patient Journey
The path to a reflux-free life begins when you decide that managing your symptoms is not solving the problem. Typically, people will attempt to first control the symptoms with diet and lifestyle changes. When that ceases to have an affect on symptoms, your doctor will suggest PPIs.
Since you can’t cure reflux with either of those steps, people often choose to have their valve restored to its original effectiveness with the TIF procedure.
In a randomized study comparing the results of PPI treatment of reflux to the TIF procedure, all patients in the PPI group opted to have TIF at the end of the six month study.7
Before your TIF Procedure

Your physician will fully prepare you for your procedure day and beyond during your consultation. A little planning goes a long way, so do arrange for transportation home after the procedure and have meals ready to go that adhere to the diet provided by your physician.
Given that your physician will be working in your esophagus and stomach, you will need to be sure your stomach is empty of food and medicines by fasting for several hours before your procedure.
During your TIF Procedure

Plastic fasteners are used to hold the tissue in place. Your body will heal around these fasteners. If you have a small hiatal hernia, this will also be fixed as part of the procedure.
After your TIF Procedure

Every person is unique, and TIF trained physicians understand this, so expect your doctor to give you specific instructions about post-procedure care based on your personal situation. You can count on needing to follow a diet that gradually moves from liquids to solids while your restored valve heals. This can take four to six weeks, depending on each individual.
Just remember during this time that you are in the homestretch!
As long as your job doesn’t involve a lot of physical exertion, you may return to work a few days after the procedure. It’s important that you not lift heavy items or do any strenuous physical exercise until your physician sees you for a post follow-up exam.
Because the procedure is gentler on the body than other traditional laparoscopic procedures, there is less discomfort, but you may experience some minor soreness in your throat, chest, and shoulder area, which will dissipate over a few days.

“My TIF procedure was almost two and a half years ago. I take no medicine for reflux, eat a wide variety of foods, and don’t reflux while exercising. I am not constantly drinking or brushing my teeth. The pain, anxious feelings, and discomfort are gone. Not a day goes by that I don’t appreciate my TIF procedure and the improvement it has brought to my life.”
—Sheldon H.
“The TIF procedure bridges the treatment gap between medication and more invasive surgery. Because surgeons perform the procedure entirely through the patient’s mouth, they make no abdominal incisions and leave no scars from the procedure.”
—Dr. Michael Murray, MD
General and Foregut Surgeon, Reflux Specialist
Northern Nevada Medical Center
Reno, NV

- In the 2 studies in 56 patients where esophagitis was assessed at >=36 months, the median follow-up was 44 months, the weighted percentage of patients where the esophagus had completely healed was 83.94%.
- https://www.gerdhelp.com/blog/references/the-tempo-trial-at-5-years-transoral-fundoplication-tif-2-0-is-safe-durable-and-cost-effective/
- In the 2 studies in 88 patients where median follow-up was 59.5 months, 78.4% of the patients stated they were satisfied with the outcome of the procedure.